Health in All Policies and intersectorality in Latin America and the Caribbean, 2011 - 2021: a scoping review
Fabio Alberto Escobar-Díaz1, Zuly Andrea Rodriguez-Corredor1.
1. Fundación Universitaria del Area Andina. Bogotá DC, Colombia.
Enviado: 8 de agosto de 2023.
Aceptado: 29 de septiembre de 2023.
Autor de correspondencia: Fabio Alberto Escobar Diaz. E-mail: fescobar13@areandina.edu.co
Abstract
Introduction. Intersectoriality, since the Alma Ata Conference in 1978, has become a fundamental part of the political discourse on public health, social determinants, and health promotion to address health problems in society. Following the above, it is important to identify the research carried out in Latin America and the Caribbean on this topic in the last decade. methods. A scoping review was carried out on the scientific evidence published between 2011 and 2021 in countries of the Latin American region on experiences and intersectoral actions between health and other sectors to address joint public health problems. Results. 15 studies were included; mostly from Brazil, with predominantly qualitative designs and local character. In addition, some analyses highlight the hegemony of the biomedical model, as well as the conflicts and tensions at the ideological level in certain health issues and traditional practices that limit effective intersectoral collaboration. discussion. Intersectoriality is not a strictly technical issue, but ideological elements converge that determine its scope and limitations. Studies in countries such as Colombia should be expanded to have evidence that allows an understanding of the barriers and facilitating aspects of intersectorality.
Keywords: intersectoral collaboration, social determinants of health, Public Policy, Latin America
Salud en todas las políticas e intersectorialidad en América Latina y en el Caribe, 2011-2021- Revisión de alcance
Resumen
Introducción. La intersectorialidad, desde la Conferencia de Alma-Ata en 1978, se ha convertido en una parte fundamental del discurso político sobre salud pública, determinantes sociales y promoción de la salud para abordar los problemas de salud en la sociedad. En relación a esto, es importante identificar la investigación que se realizó en América Latina y en el Caribe sobre este tema en la última década. Métodos. Se realizó una revisión de alcance sobre la evidencia científica publicada entre 2011 y 2021 en países de la región latinoamericana sobre experiencias y acciones intersectoriales entre salud y otros sectores para abordar problemas conjuntos de salud pública. Resultados. Se incluyeron 15 estudios, en su mayoría de Brasil, con diseños predominantemente cualitativos y de carácter local. Además, algunos análisis destacan la hegemonía del modelo biomédico, así como los conflictos y tensiones a nivel ideológico en ciertos temas de salud y prácticas tradicionales que limitan una colaboración intersectorial efectiva. Discusión. La intersectorialidad no es un tema estrictamente técnico, sino que convergen elementos ideológicos que determinan su alcance y limitaciones. Deben ampliarse los estudios en países como Colombia para contar con evidencia que permita comprender las barreras y los aspectos facilitadores de la intersectorialidad.
Palabras clave: Colaboración intersectorial, Determinantes sociales de la salud, Política Pública, América Latina.
Introduction
Since the Declaration of Alma-Ata in 1978 on Primary Health Care (PHC), intersectorality has gained prominence at the international level to act in favor of improving health conditions in societies. With the Ottawa Charter in 1986 on Health Promotion and more recently with the approach called Health in All Policies (HiAP), the importance of intersectorality in policies that allow maintaining and protecting health has been emphasized, due to the impossibility of solving problems exclusively from this sector (1).
However, intersectorality still lacks an unequivocal and agreed definition, nor does it have a structured theoretical basis, and the study or systematization of how it has been practiced is still very scarce. Different similar terms that are used as intersectoral action, dialogue, or collaboration, agree that public health policies that commit to other sectors must also consider their impact on their social determinants at the population level (2). Intersectorality, in general, refers to the integration of various sectors to comprehensively solve social problems, which implies having the articulation between their bases, both political ( construction and implementation of joint policies and strategies between the sectors) as technical (share resources and specific knowledge of each sector to achieve better solutions) (3).
Intersectorality proposes a new rationality in public management that seeks to overcome the fragmentation of policies, considering the concept of health as a whole, and that offers a different way to plan, implement, and monitor the provision of services by the different sectors (3). However, in practice there are different visions or ways of developing intersectorality, focusing on some aspects more than others. For example, some emphasize that the other sectors must incorporate equity and respond to health needs; others, instead, focus on collaboration between governmental and non-governmental sectors; Some of the definitions even find intersectoriality as a modality of work articulated between the public and private sectors (4).
The HiAP approach was first coined in the late 1990s and has been promoted from within the European Union (2). It was used at the 8th International Conference on Health Promotion in 2013, where the slogan “Health in All Policies” was used (5) and proposes that the sectors in which the state operates must take into account the meaning of health in their own decisions, to build synergies that favor health or avoid negative impacts on the population (6). Therefore, HiAP is considered the mechanism to act on the social determinants of health (SDH) (7).
A literature review was carried out, using the scoping review method. To map and describe the scientific evidence that exists on intersectoral actions in health, including those under the HiAP approach, in Latin American and Caribbean (LAC) countries, the review question formulated was: what are the studies and research carried out on Intersectorality and HiAP in LAC in the period 2011-2021? Therefore, all Spanish and Portuguese-speaking countries at the continental and insular level were considered: Argentina, Bolivia, Brazil, Chile, Colombia, Costa Rica, Cuba, the Dominican Republic, Ecuador, El Salvador, Guatemala, Honduras, Mexico, Nicaragua, Panama, Paraguay, Peru, Puerto Rico, Uruguay and Venezuela.
Methods
A scoping review was developed to map and characterize different studies carried out in LAC that address intersectoral experiences and actions in health or from the HiAP perspective. The scoping review is a type of review that does not attempt to address such specific questions to identify interventions, but instead explores the breadth and depth of the existing literature, maps and summarizes the evidence, and guides future research (8). The review process was developed by the two researchers independently.
The bibliographic databases Pubmed, Scopus, Scielo, and Web of Science were chosen. Terms indexed in the Descriptors in Health Sciences (DeCS) and Medical Subject Headings (MeSH) and free terms were used: collaboration, action or intersectoral work, intersectorality, social determinants of health, public policies, health in all policies, and their equivalent in English such as intersectoral collaboration, intersectoral action, social determinants of health, public policy, health in all policies. For the combinations between the terms, we use the boolean connectors AND and OR. With the relatively small number of records found in the different databases, it was not necessary to include terms related to LAC countries, but their identification was done manually.
The inclusion criteria used were the following: a. Research articles or originals from LAC countries, published in Spanish, English, and Portuguese; b. Studies whose main objective addresses Intersectorality or the HiAP approach; c. That they have been carried out in the period 2011 – 2021. In addition, only those that were open access were accessed. All records that did not meet the above criteria were excluded.
The search was carried out between July and October 2022. The records found in each database were exported and sent to the Rayyan® platform from where the researchers excluded duplicates as well as screened by title and abstract. Of 1242 records found in the 4 databases, 728 remained after excluding 514 because they were duplicates. Of the 728 by title and abstract, 52 were filtered. Of these eligible, 37 were excluded because they were outside the analysis period, did not address intersectorality as the central objective of the study, or belonged to a population or geographic location other than LAC. Finally, 15 studies were included in the review.
Results
A total of 15 studies were included in the scoping review (Figure 1). One of the first results to highlight is that the majority of studies on intersectorality and HiAP in LAC have been carried out, within the period 2011-2021 in Brazil, with 11 investigations published in scientific journals. Colombia follows in their order with 2 and Chile with only 1. As a particular case, there is a study that analyzed nutritional policies in Latin American countries and that incorporates an analysis of intersectorality (Table 1).
Figure 1. PRISMA study selection flowchart
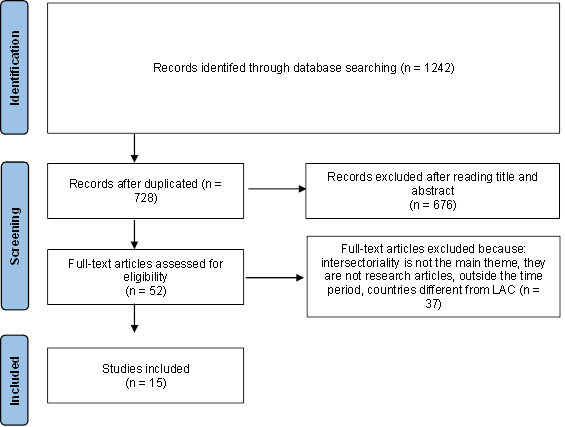 |
Table 1. Characteristics of studies included, HiAP and Intersectorality in LAC, 2011-2021
|
Authors |
Year |
Country |
Methods |
Population |
Sample |
|
Aguiar et al.(9) |
2020 |
Brazil |
Qualitative |
Professionals from Primary Health Care teams |
intentional |
|
Andrade, et al.(10) |
2018 |
Brazil |
Quantitative |
Representatives of institutions that promote free physical activity in communities |
intentional |
|
Arches, et al.(11) |
2016 |
Chile |
Qualitative |
Professionals from a primary-level family health center and the social sectors involved |
intentional |
|
Babajide, et al.(12) |
2021 |
Colombia |
Qualitative |
Cities that have implemented mass public transport systems (BRT) in the world |
intentional |
|
Barros, et al.(13) |
2020 |
Brazil |
Qualitative |
Policymakers and legislation in the field of occupational safety and health, managers, and those responsible for its implementation in Sao Paulo in the health, work, social welfare, and justice sectors |
intentional |
|
Chiari, et al.(14) |
2018 |
Brazil |
Mixed |
Municipal Managers of the School Health Policy |
intentional |
|
Dias, et al. (15) |
2018 |
Brazil |
Qualitative |
Program administrators at the municipal level, health area managers, primary care professionals, municipal education managers, and school professionals involved with the program |
intentional |
|
Lencucha et al.(16) |
2013 |
Brazil |
Qualitative |
Parliamentarians, authorities from key ministries, representatives of civil society, and intergovernmental bodies |
intentional |
|
Molina, et al.(17) |
2018 |
Colombia |
Qualitative |
Health professionals and leaders of community health organizations in six cities. |
intentional |
|
Nunes, et al.(18) |
2019 |
Brazil |
Qualitative |
Professionals linked to the intersectoral mental health network of a municipality |
intentional |
|
Pinheiro et al.(19) |
2017 |
Brazil |
Qualitative |
Nurses and doctors from four family health teams and teachers from a municipal primary school. |
Intentional |
|
Pinho et al. (20) |
2017 |
Brazil |
Qualitative |
Teams, managers, users, and relatives around mental health care services |
intentional |
|
Pinto, et al.(21) |
2019 |
Brazil |
Qualitative |
Members of the community network that promotes educational, care, and health actions (schools, basic health units, social assistance centers) and NGOs |
intentional |
|
Pinto, et al.(22) |
2020 |
Brazil |
Qualitative |
Public school teachers in a Brazilian municipality |
intentional |
|
Tirado, et al.(23) |
2016 |
Latin America |
Qualitative |
Latin American countries |
intentional |
On the other hand, 13 of the 15 articles have qualitative methodologies where they use different information collection strategies such as individual semi-structured and in-depth interviews. Only one is quantitative and another has a mixed methodological design. Regarding the sample, taking into account the qualitative nature of most of the studies, they used a non-probabilistic and intentional, or purposive, sampling, consistent with the objective of each research.
Table 2. Objectives of the studies, main results, and sectors considered.
|
Authors |
Objective |
Main results |
Sectors considered |
|
Aguiar et al. (9) |
To analyze the changes produced in the assistance services (psychosocial, police, and judicial) of the intersectoral network of care for women |
● Greater knowledge of professionals about the existence of other services ● Better perception of the difficulties of integration between services ● There are more services but they are segmented ● Ideological, religious, and gender differences hinder communication and the integration of services. |
Health, Justice, Social assistance |
|
Andrade, et al.(10) |
To describe a local physical activity promotion network |
● 40% of relationships in the network only exchange information ● 20% were collaborative or association relationships ● The public sector concentrated 40% of the associations and alliances in the networks |
Recreation and sport |
|
Arches, et al.(11) |
To understand the experiences lived by professionals in the management of processes of the Comprehensive Child Protection System in a location of the Metropolitan Region, Chile |
● Lack of linkage of the policy guidelines with the local context and the demands of the population ● Resistance to change or innovation due to a perception of increased workload with more responsibilities ● The hegemony of biomedical discourse ● The predominance of the pragmatic, the economy of effort and time, the routine and familiar |
Health, social assistance |
|
Babajide, et al.(12) |
To examine SDH, equity, and intersectoral approaches and their incorporation into the local political process around the BRT (Bus Rapid Transit Systems) policy, in 3 megacities: Lagos, Bogotá, and Bejing |
● Policy decisions on BRT rarely take into account its health impacts ● Limited data to guide policies or assess their impact on health. ● Health ministries do not participate in politics ● Health experts were not linked to BRT policies
|
Transport |
|
Barros, et al.(13) |
To know the perspective of the formulators and managers of public policies aimed at workers at the municipal, state, and national levels, concerning the intersectorality |
● Intersectorality is not natural or spontaneous ● The sectors do not know the roles of others, nor are their actions or experiences shared. ● There are no joint strategies to address the problems ● Excessive emphasis on the specificities of each sector that do not favor unity or collaboration. ● Information is shared but coordinated actions and solutions are not ● Intersectorality is perceived more as an individual or private initiative, not institutionally supported. ● Productivity and the organization of sectoral actions are privileged because they are routine, controlled, and measurable. |
Health, work, social welfare, justice |
|
Chiari, et al. (14) |
To evaluate the implementation and execution of the Health at School program (PSE) in the municipality of Belo Horizonte, Minas Gerais |
● The implementation of the PSE has not managed to adopt a logic of intersectoral action ● PSE does not promote integration and articulation between sectors and actors ● It does not have decision-making power, nor does it have institutional support ● There is no alternation in the coordination of the intersectoral space, assumed only by the education sector. ● Imposition of only one sectoral vision of an intersectoral program ● The permanence of the biomedical intervention model with a traditional pattern of isolated actions |
Education and health |
|
Dias, et al.(15) |
To identify and analyze the process of building intersectoral arrangements between the health and education sectors, in particular the institutional and management spaces, the negotiation processes, the convergences, and the ideas in dispute, in the context of the implementation of the NutriSUS strategy in a city in the State of Rio de Janeiro. |
● Intersectoral management is encouraged locally but without sustainability due to the predominance of the sectoral tradition and one sector in the programs. ● The design of the program and the participation of the sectors and actors did not favor pedagogical integration ● Some preventive actions are not favorable for building intersectorality since they are sectoral measures. ● There is no articulation between the principles of the health program and the education program, one from a medicalized vision (iron supplement) and the other from a social, economic, and environmental vision (food). ● Intersectoriality depends on managers' initiative and willingness to dialogue and negotiate ● The education sector participates only in the execution and operationalization of the program, not in its conception or design. |
Education and health |
|
Lencucha et al.(16) |
To examine the institutional characteristics of the National Commission for the Implementation of the Framework Convention for Tobacco Control, its institutional characteristics that facilitated or impeded its ability to promote intersectoral tobacco control |
● Norms and rules for government-industry interaction and cross-sector tobacco control across all sectors ● Better consistency in favor of tobacco control from actors who were against these measures ● The Commission facilitates the rules and regulations of the game that promote and protect the government's ability to create tobacco control legislation. ● Some of its members have direct relationships with the tobacco industry and defend its interests. ● Divergence of perspectives between tobacco as an economic good (production, industry, trade, employment) and public health |
Parliament, Health, Foreign relations, Commerce and industry, Agriculture |
|
Molina, et al.(17) |
To understand the aspects involved in decision-making in public health policies and programs and their relationship with access and quality of these programs |
● Short-term intersectoral articulation or cooperation experiences in specific programs and projects ● Intersectoral experiences are manifested through: alliances, contracts, agreements, pacts, tables, acts of commitment, and community diagnoses. ● Some facilitators of intersectorality are: a shared vision of the problem, national guidelines, continuity of suitable personnel, the political will of the ruler, support from secretaries of finance and planning ● Some tensions and difficulties regarding intersectorality such as weak ability to convene authorities, lack of consideration for local knowledge, private or individual initiative, non-institutional, interpersonal conflicts, competition or rivalry between actors, distrust, language and communication problems between politicians and technicians, passive resistance, disjointed, complex and inconsistent regulations, incompatibility of schedules and times |
Health, Education, Childhood, Culture, Recreation and Sport, Treasury |
|
Nunes, et al. (18) |
To analyze the possibilities and challenges in building intersectoral networks in mental health |
● Need to establish alliances with other health services and other sectors: family, school, and recreation. ● The predominance of the biomedical model in psychosocial health care focused on the institution, disease, and pharmacology. |
Health, Justice, Social assistance, and education |
|
Pinheiro et al.(19) |
To analyze how the work of sexual education for adolescents and young people is developed from the perspective of the intersectoriality between health and education |
● Predominant responsibility towards the health professional ● Lack of intersectoral integration ● Teachers have not updated their speeches on sex education. ● Teachers do not have professional preparation to address issues related to sexuality. ● Fragmented sectoral organizational structure and the existence of power relations between sectors. ● There are no concrete intersectoral actions for the development of sexual education work for young people and adolescents. |
Health and education |
|
Pinho et al.(20) |
To evaluate intersectoral resources in the composition of networks for the care of crack users |
● There is no intersectorality. There is no networking with the judicial authorities such as the Prosecutor's Office or the military brigades. ● The gateway to the care network is through the legal apparatus and not the health system. ● A stigma-based, prohibitionist and criminal political view of crack use predominates, not a public health view. The user is considered a criminal, not a sick person ● Little articulation with actions not related to health at a social, recreational, or cultural level as part of support and therapeutic measures for the consumer |
Health, Justice, Social assistance |
|
Pinto, et al. (21) |
To analyze the health promotion actions of a territory, seeking to answer how they reveal the values, principles, and guidelines of the national health promotion policy |
● Participation is restricted because the community is not involved in the planning or evaluation of the actions ● The network has institutional but not community interests ● The network reproduces the traditional concept based on assistance ● The preventive and hygienist, clinical, and biomedical logic predominates in health actions. |
Social assistance, education, health, community |
|
Pinto, et al.(22) |
To analyze discourses, representations, and approaches to health and health promotion in schools |
● The hegemony of the health, clinical, and biological medical model in the discourse and social practice of public school teachers ● Teachers separate health from its social determinants and hold the person responsible for their health. ● Health promotion is assumed as risk prevention through changes in behavior |
Health and Education |
|
Tirado, et al.(23) |
To map existing policies that address malnutrition in all its forms in Latin America |
● Nutritional actions have been incorporated into social protection and food security policies in the education, environment, agriculture, and employment sectors in some countries. ● Policies lack intersectoral integration to promote nutrition and prevent non-communicable diseases |
Health, education, environment, agriculture |
The studies included in our review reflect some characteristic elements to understand intersectoral experiences or health action in sectors other than this one. Although they did not have an evaluative scope, most of them reflect difficulties and problems for effective intersectoral action. Here, in some of these studies, it was reflected how the biomedical, clinical, and preventive model that is based on the disease as a point of action may be limiting intersectoral action given the impossibility of generating consensus or agreements with other sectors (18, 21, 22).
second aspect to consider in the analysis of these studies is that the action of the State seems to be traditionally separated between the different sectors, where each public institution that represents a sector has its programs or actions and there is resistance to work articulately. The study on the BRT (12) or related to school health (14,15), where sectors such as mobility, transport, and education operate in a sectoral way with many difficulties to recognize the role of the health sector in their programs or policies.
On the other hand, the different ideological positions can negatively affect the construction of intersectoral collaboration. Issues such as the consumption of psychoactive drugs, sexual and reproductive health, and the gender approach (19,20) generate tensions because they reflect different positions and beliefs among people. After all, sectors other than health maintain traditional positions on them. These conflicts in the ideological terrain also constitute a significant limitation for intersectoral action.
In connection with the above, intersectorality faces practices specific to each sector in terms of performance and activities that the officials of the institutions carry out daily. In this way, working collaboratively between sectors can generate resistance due to the perception of greater workloads, commitments, and responsibilities than they usually have, acting only individually, institutionally, and sectorally (13).
However, concerning the sectors linked to or considered in the studies included in this review, those who investigate intersectoral collaboration between health and education seem to have more interest in areas such as health promotion, sexual education, and nutrition (14)(15)(19). There are very few research which integrate sectors such as transportation (12) or physical activity into their analysis. (10). The studies that include the justice sector are remarkable, especially in problems related to violence against women, mental health, and the consumption of psychoactive substances (9,18,20).
Discussion
This scoping review aimed to map the scientific literature on studies that examine intersectorality and the HiAP approach in LAC countries, in the period 2011-2021. The analysis of the 15 studies that were included shows that: 1. Brazil is the country that has carried out and published the most studies on intersectorality in health in the Latin American region; 2. Almost all the studies are qualitative, with intentional or non-probabilistic samples ; 3. There is only quantitative research; 4. Effective intersectoral action is extremely complex to carry out; 5. The predominance of the preventive and biomedical models can limit intersectoriality; 6. The ideological aspects around certain public health problems in conflict represent a challenge to build intersectoral actions and; 7. Resistance to change, innovation, and uncertainty in the face of collaboration between sectors is a barrier to these joint initiatives.
Among the studies reviewed, it is notable that none of them address the HiAP approach, but conceptually they are based on intersectorality, work, or intersectoral action. According to Panamerican Health Organization (PAHO) (4), HIAP has been promoted mainly in countries with significant capacity to regulate markets, coordinate the provision of social services, and implement redistributive policies through taxes or other mechanisms, aspects that do not occur in most LAC countries, with more limited capacities.
On the other hand, the small number of studies that were included in our review is consistent with what Shankardass (24), and PAHO had previously pointed out (4), in that the growing interest and use of intersectoral actions have not gone hand in hand with research addressing their implementation, in terms of their success or failure. A review of the international literature carried out in 2018 by Corbin (25) responded to the objective of identifying alliance processes on health promotion, finding 26 studies carried out between 2007 and 2015, a period of 8 years, mostly from the United States, and none on LAC. Another similar review about health promotion was developed by Reza (26) in 2021 to map the existing literature between 2001 and 2015 about intersectorality and the HIAP approach and finding 52 articles in the review according to the established inclusion criteria; most studies come from the United States, again, and to a smaller extent, from Germany, Canada, and Australia. Among the LAC countries, only Brazil is found, with only one study. Of the 52 studies, 27 were classified as public health, 6 as mental health, and 6 as school health.
Gugliemin and other researchers (27) developed a scoping review on the implementation of the HiAP approach at the local level between 2002 and 2016. Most of the studies that entered the review come from North America and Europe, 14 out of 23 articles, and none of them come from any LAC country. The authors argue that the scarce scientific evidence on HiAP is because it is a relatively recent topic.
In conclusion, it is important to advance and strengthen research in all LAC countries, specially in those with lower production on experiences and actions of an intersectoral nature. This is necessary to address, from the perspective of Social Determinants of Health (SDH) and health promotion, public health problems of populations both locally and nationally. These studies could generate evidence to guide and strengthen decision-making around policies under an SDH approach. Besides, is desirable to do more research addressing mixed methodologies, combining quantitative or qualitative analysis, whose results would contribute to a better comprehension of intersectoriality, its limits and requirements facing ideological aspects or particular bureacratic dynamics in each sector.
References
1. Diez E, Camprubí L, Ferreli R. Recommendations with technical and operational guidelines for strengthening the Intersectoral Public Health Commission in Colombia. Bogotá DC: Eurosocial, Public Health Agency of Barcelona, Ministry of Health and Social Protection; 2015.
2. Pan American Health Organization. Intersectorality and equity in health in Latin America: an analytical approach. Washington, DC: PAHO; 2015.
3. Solar O, Valentine N, Rice M, Albrecht D. Moving forward to Equity in Health: What kind of intersectoral action is needed? An approach to an intersectoral typology. Nairobi: 7th Global Conference on Health Promotion; 2009.
4. Pan American Health Organization. Intersectorality and equity in health in Latin America: an analytical approach. Washington, DC: PAHO; 2015.
5. World Health Organization. Health in All Policies: Framework for Country Action. Geneva: WHO; 2015.
6. Sanz-Tolosana E. Health in all policies. Notes for action. Aposta Journal of Social Sciences [Internet]. 2015;(66):122–47. Available from: http://www.redalyc.org/articulo.oa?id=495950262006
7. Baum F, Lawless A, Delany T, Macdougall C, Williams C, Broderick D, et al. Evaluation of Health in All Policies: Concept, theory, and application. Health Promote Int. 2014 Jun 1;29(S1):i130–42.
8. Peters M, Godfrey C, McInerney P, Munn Z, Tricco A, Khalil H. Chapter 11: Scoping Reviews (2020 version). In: Aromataris E, Munn Z, editors. JBI Manual for Evidence Synthesis. Joanna Briggs Institute; 2021.
9. de Aguiar JM, D'oliveira AFPL, Schraiber LB. Historical changes in the intersectoral network of services targeted at violence against women – São Paulo, Brazil. Interface: Communication, Health, Education. 2020;24:e190486.
10. Andrade DR, Garcia LMT, Perez DCP. Local collaborations for physical activity promotion: A network analysis. Cad Saude Publica. 2018;34(10):e00127517.
11. Arcos-Griffiths E, Vollrath-Ramírez A, Muñoz-González LA, Sánchez-Segura X. Understanding the management of public policy for the comprehensive protection of children in Chile. Rev Gerenc and Polit Salud. 2016 Jul 1;15(31):51–62.
12. Babajide O, Martins DC, Maani N, Abdalla SM, Gomez EJ, Pongsiri MJ, et al. Improving Decision-Making for Population Health in Nonhealth Sectors in Urban Environments: the Example of the Transportation Sector in Three Megacities—the 3-D Commission. J Urban Health. 2021 Aug 1;98(Supp 1):S60–8.
13. Barros J de O, Daldon MTB, Rocha T de O, Sznelwar LI, Lancman S. Intersectoriality in health and work in the current Brazilian context: The utopia of reality? Interface: Communication, Health, Education. 2020;24:e190303.
14. Chiari APG, Ferreira RC, Akerman M, Amaral JHL do, Machado KM, Senna MIB. Intersectoral Networks of the Health Program at School: perceptions and practices. Public Health Cad. 2018;34(5):e00104217.
15. Dias PC, Henriques P, Ferreira DM, Barbosa RMS, Soares DSB, Luquez TM de S, et al. Challenges of inter-sector collaboration in public policies: The dilemma between nutritional supplementation and the promotion of healthy eating in schools. Cad Saude Publica. 2018;34(12):e00035218.
16. Lencucha R, Drope J, Bialous SA, Richter AP, da Costa E Silva VL. Institutions and the implementation of tobacco control in Brazil. Cad Saude Publica. 2017;Sup 3:e00168315.
17. Molina-Marín G, Ramírez-Gómez A, Oquendo-Lozano T. Inter-sectoral and inter-institutional cooperation and coordination in public health within the market model of the Colombian health care system, 2012-2016. Public Health Magazine. 2018 May 1;20(3):286–92.
18. Nunes CK, Olschowsky A, Silva AB da, Kantorski LP, Coimbra VCC. Mental health in children and adolescents: a vision of the professionals on challenges and possibilities in building up intersectoral networks. Rev Gaucha Enferm. 2019;40:e20180432.
19. Pinheiro A de S, Silva LRG da, Tourinho MBA da C. The health strategy of the family and the school in sexual education: an intersectoral perspective. Work, Education, and Health. 2017 Dec;15(3):803–22.
20. Pinho LB de, Wetzel C, Schneider JF, Olschowsky A, Camatta MW, Kohlrausch ER, et al. Evaluation of intersectoral resources in the composition of care networks for crack users. Anna Nery School. 2017 Oct 26;21(4):e20170149.
21. Pinto MB, Silva KL. Health promotion in the territory: strengths and challenges of local projects. Anna Nery School. 2019;23(1):e20180282.
22. Pinto MB, Silva KL. Health promotion in schools: speeches, representations, and approaches. Rev Bras Enferm. 2020;73(3):e20180774.
23. Tirado MC, Galicia L, Husby HB, López J, Olamendi S, Chaparro MP, et al. Mapping of nutrition and sectoral policies addressing malnutrition in Latin America. Rev Panam Public Health. 2016;40(2):114–23.
24. Shankardass K, Renahy E, Muntaner C, O'Campo P. Strengthening the implementation of health in all policies: A methodology for realist explanatory case studies. Health Policy Plan. 2015 May 1;30(4):462–73.
25. Hope Corbin J, Jones J, Barry MM. What makes intersectoral partnerships for health promotion work? A review of the international literature. Health Promote Int. 2018 Feb 1;33(1):4–26.
26. Reza Amir Esmaili M, Damari B, Hajebi A, Rafiee N, Goudarzi R, Haghshenas A. Basic Criteria, Models, and Indicators of Intersectoral Collaboration in Health Promotion: A Scoping Review. Iran J Public Health [Internet]. 2021;50(5):852–65. Available from: http://ijph.tums.ac.ir
27. Guglielmin M, Muntaner C, O'Campo P, Shankardass K. A scoping review of the implementation of health in all policies at the local level. Vol. 122, Health Policy. Elsevier Ireland Ltd; 2018. p. 284–92.